by Philip Boxer
The different kinds of value proposition at the edge involve different kinds of relationship to the user as follows 1:
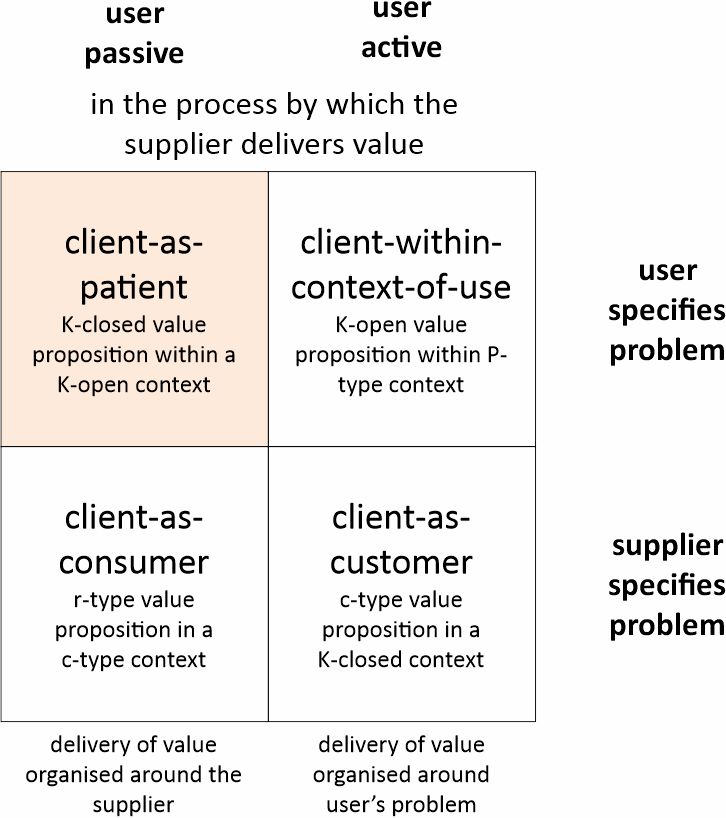
With r-type propositions, there is no relationship to the user’s situation, the user being reduced to a ‘consumer’. With c-type propositions, the way the product or service is delivered can be customised to fit into the user’s situation, making the user a ‘customer’. In both these cases, the supplier specifies the nature of the problem that it will deal with.
This changes with K-closed and K-open propositions. Here the user specifies the problem, which may be no more than a P-type ‘pain’ that needs identifying (K-open) before it can be defined as a particular kind of problem (K-closed). Once defined, the supplier then has to orchestrate and synchronise (align) a number of products and services to deal with it. This makes the user a ‘client’. A special case of this arises when the products and services that are available to be aligned are constrained by what the supplier is able to make available. This reduces the user to a ‘patient’.2
Notes
[1] The original version of this two-by-two was in a paper by myself and Robin Wensley in 1996, entitled: Is the customer an endangered species? Niches and Clusters
[2] Doctors are, or course, trained to approach their ‘users’ as clients. Where they are constrained in the kinds of treatment they can align to the user’s condition, whether by their own knowledge or by the infrastructure they are able to draw on, then the user can be reduced to being a patient. Much benefit is derived, however, from the user’s active involvement with their condition – particularly if the condition is chronic. The current dilemma facing the NHS, therefore, is how to create the conditions where this active involvement is possible.